
On the Farm
I took Ada to pet the new lambs at a local farm. She wanted to babywear too, so here we both are, wrapped up on the farm:


I took Ada to pet the new lambs at a local farm. She wanted to babywear too, so here we both are, wrapped up on the farm:
Babywearing, and nursing, at the Florida State Fair:

Nursing on the Ferris Wheel

Goat, Annabelle, and I

Sideways in the Front Cross Carry
Above you can see where I put Annabelle in the front cross carry sideways. I figured it would give her a view while still supporting her in a physiologically safe way, and giving her a way to cuddle against me before she became overstimulated. I think it’ll work great, but the fact is that right now all she wants to do, especially in a noisy public place, is nurse. So she soon ended up tummy to tummy again. Also known as mouth to nipple.
Once or twice we ended up stuck behind a clunky stroller trying to maneuver through the muck of the fair. I was glad not to be so burdened, and also not to be burdening my fellow fair-goer!
I love our local weekly moms group (and if you live anywhere near Pinellas County Florida you’re invited–Wednesday’s at 11am at the Dunedin Labor of Love). It is so much fun to hang out with a group of strong women and happy babies and be able to ask questions of and discuss topics with the kind of people whose answers you respect and appreciate!
And I get to wrap with other moms. Sometimes I’m showing them the ropes (showing them the wraps?), sometimes we’re just having fun. Wrapping is fun, but wrapping in good company is better:

Getting wrapped up together!

Our babies are in the same position as when they were in the womb!
Sometimes when I’m showing someone how to adjust the wrap behind them, I run into this problem that they simply cannot reach as well as I can. So I had to learn a new way to wrap up a little baby in a high back carry. A way to do it without reaching high up my back.
Today I experimented with a rucksack. I found that I could do the entire carry, bringing the straps over and under the legs, while my 7 week old baby was very low on my back. Then a few bouncing tugs on the tails hiked her up to my neck. Voila!
I’m so good, I even had it together to make a video!
A (well meaning) friend asked with concern whether Annabelle sleeps outside the wrap since “it just seems like such a comfortable place to sleep!”
I hastily assured her that Annabelle sleeps just fine in her cradle by day and in our bed at night. “But not on me,” I assured her. I was quick to defend babywearing from the implication of spoiling babies. But upon reflection, I wonder at this obsession with not letting babies get too attached, and I wish I could say that I had answered, “I don’t know how she would sleep without me and I’m not interested in finding out!”
We don’t have to teach infants independence. They’re incapable of independence– they rely on us completely. As they become capable their independence will spring from the knowledge of security in our love and support. Do we want to teach our children that they can sooth themselves by demonstrating that they survive our neglect, or do we want them to learn self-soothing from our loving example?
The fact is that infants are designed to be on their mothers constantly. Mother and baby thrive this way and the more devices and conveniences separate a baby from his mother, the more benefits are lost.
Perhaps if our culture could shift the emphasis in child rearing away from convenience and toward constant nurturing, we might discover the “convenience” of satisfied, thriving babies; of children who completely trust parents; of neighbors, co-workers, and politicians who have all benefited from an early introduction to a love-filled world . . .
I’m not recommending martyrdom. In fact, I experience relief from pressures when I remind myself not to worry about my actions “spoiling” my child by allowing her to become accustomed to sleeping in-arms, nursing-on-demand, and having her every newborn whim catered to as best I can. Once I let those considerations go, I find that I am free to delight in the constant sight, smell, sound, and feel of my baby. I am free to neglect the dusting, let the machine answer the phone, and wear the same outfit I wore yesterday. I am free to spend hours relaxing with my baby and I find that catering to her every whim provides an enjoyment and satisfaction beyond anything I could get done while she naps in the cradle.
I’m not going to waste my time worrying that she’ll never learn to sleep by herself. People all across the globe and throughout history have managed it.
Just my opinion but the only “spoiled” baby is the one whose babyhood is wasted on sleep training and feeding schedules. Even then, the baby isn’t spoiled–it’s really just the time together that’s been spoiled. And there’s no getting that time back.


The term is brand new to me, but it turns out I already practice ecological breastfeeding!
I came across it in my search for an acceptable birth control method. Ecological breastfeeding is free, comfortable, and natural–it fits all my criteria!
Wikipedia reports that it has a 1% failure rate in the first six months of a baby’s life, and only 6% failure rate after that until the woman’s period returns. Pretty good rates for something I was doing anyway.
According to Wikipedia:
I don’t nap with Annabelle (I would if I didn’t have a five year old to keep up with) but she does nap on me, and I assume it is the proximity, not the sleep, which contributes to the effectiveness of ecological birth control.
And so I have discovered another benefit to the family of babywearing: it contributes to convenient spacing of babies and helps avoid the use of dangerous or inconvenient birth control methods!
Does it seem to anyone else that so many “modern conveniences” (strollers, pacifiers, cribs, and bottles) end up being more of an inconvenience than anything else?

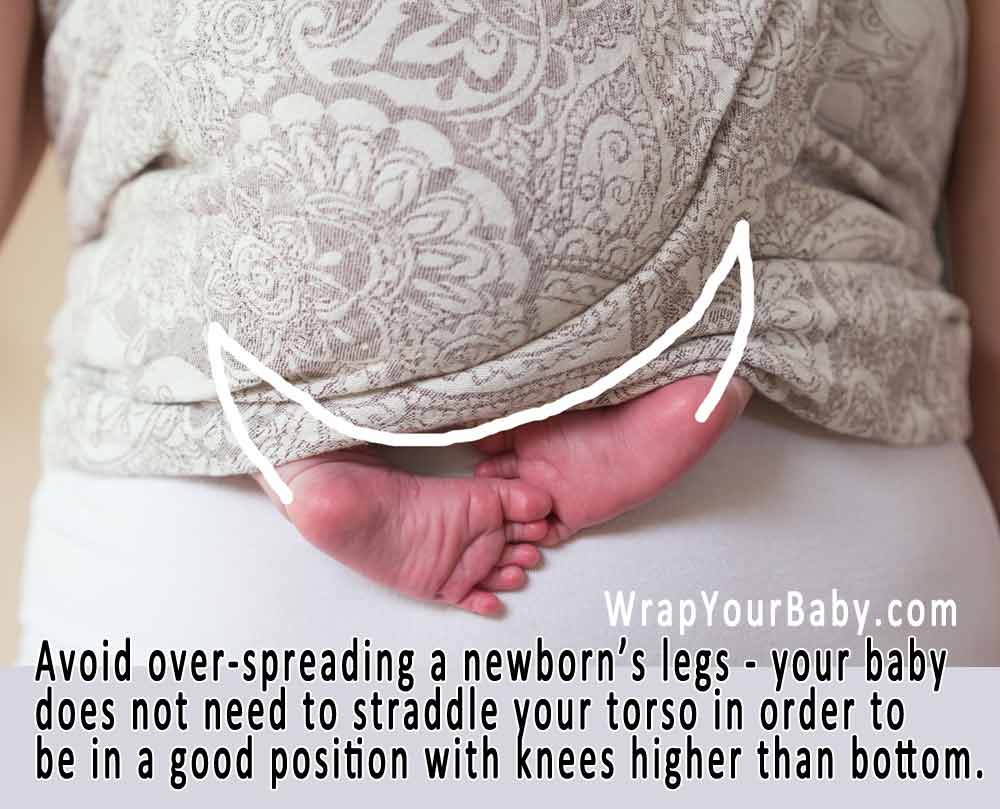
Wondering whether to wrap your newborn legs in or legs out?
The real question of legs in/legs out is how best to support YOUR newborn in a comfortable and ergonomic way.
Optimum newborn positioning includes:
You should wrap around baby in a position that your newborn’s legs are naturally inclined to rest in. You will find that baby will tuck knees up, not spread too far apart.
Usually you can wrap around your newborn baby with legs out while maintaining this natural position.
Baby does not need to be able to spread legs wide or straddle your torso. In fact, newborn legs are so tiny that the length of thigh from bottom to knee fits in front of a mama’s tummy with only a slight spread.
Wrapping a newborn with legs out is often more comfortable for baby.
And with newborn legs out, you can view baby’s feet to monitor circulation.
In the photos below you can see that Annabelle’s legs do not have to stretch around my waist or spread wide across my torso–she’s 6 weeks old in these pictures, and I’m wearing her low in the second picture because she’s been nursing in the front wrap cross carry.

Newborn legs don’t have to straddle your waist!
Before 2010, it was most common (among US and European babywearers) to wrap a newborn baby with legs in – inside the wrap – in what was referred to as “froggy leg” position.
Because of this, there are a lot of older photos, videos, and resources that show this style of legs-in newborn babywearing.
There’s nothing wrong with wrapping a newborn with legs in the wrap – as long as you are doing safe positioning.
So make sure baby’s knees are not spread too wide.
Make sure baby’s weight is not on baby’s feet.
Make sure baby’s feet are comfortably flexed.
Sometimes newborns are very accustomed to being curled up. And if that is what your baby’s body seems to want to do, go with it!
Here’s an example of a newborn who was not uncurled enough to wrap with legs out, but whose little feet did stick out:
Learn more about how to wrap your newborn baby here!
In conclusion, do what works best for you and your baby in terms of leg position. Newborn legs in or legs out, either way is fine.
I love our mei tai but I NEVER wear it because I REALLY love our wraps!
Someone at our mom’s group asked me to demonstrate the mei tai, so I put Annabelle on my front. I’m glad I got a picture of her in there–don’t know when she’ll be in there again!
The mei tai is very comfy, though. I put her in with her legs tucked in.
This is our very first mei tai. A Freehand Mei Tai made by Kaire when she still owned her business. Love it!

6 week old Annabelle in the Mei Tai
I recently watched the Happiest Baby on the Block DVD which offers five techniques to calm a crying baby:
swaddling
side or stomach lying
shushing, or white noise
swinging/bouncing and
sucking
If the author is correct that these five things trigger a baby’s calming instinct, it does explain why so many of us have had such fine results with wrapping which holds our babies close like a swaddle; which presses our baby’s tummy against our bodies just as with a stomach lying position; which exposes our baby to the constant sounds of our heartbeat, breathing and intestinal machinations; which bounces our baby with incessant human motion; and which contributes convenience to nursing-on-demand.
I say he’s on to something!
I felt great after Annabelle was born (perhaps due to consuming the placenta?) and was eager to go out with her after the first few days. I wanted to show that baby off!
I turned to the front cross carry for a poppable, pretied carry. It is perfect! I tie it on at home and often use it to carry Annabelle to the car when I need my hands for the diaper bag, snacks, jackets, library books, etc. I take her out and put her in the carseat, leaving the front cross carry tied on me. When we park, I take Annabelle out of her seat and pop her into the wrap without retying. I do adjust depending on whether she wants to nurse or not—for nursing I usually wear her in it upright but a lot lower so that her mouth lines up with my breast.
When we get back to the car it’s the same routine—pop her out and into the carseat. When we get home, pop her back in so I can carry groceries, bags, etc.
The front cross carry is often touted as being the much more poppable carry over the front wrap cross carry, but I have found FWCC to also be easy to pop my newborn in and out of. There is one additional pass of the wrap with the FWCC, so that means three pockets to sort out putting the baby into, but this has not been difficult.
However, I eventually settled on the front cross carry as my preferred out and about carry and this is why. First, the knot is tied in the front, so that I am not leaning back on a big old knot while driving. Of course, one could use a longer wrap for the FWCC and bring it around to the front to tie and solve that problem. Second, the FCC is very easy to tie on without your baby, and approximate the fit so that there is little adjusting needed when you do slide your baby in. With the FWCC, I need to have baby in it when I tie it.
Another carry that I love for poppability is the hip cross carry. This one could also be tied on without baby and fit fairly well with little adjustment. However, with a newborn nursing almost constantly, I prefer the discretion offered by the cross carries. A one shouldered carry like the hip cross carry just doesn’t provide adequate cover. I use it for nursing at home, but despite being a fairly unashamed breastfeeding mother, I want more modesty at the grocery store. The hip cross carry is fairly discreet when nursing on the same side that the wrap goes over my shoulder, but when we inevitably switch, I’m feeling too much of a breeze! Nursing in the HCC in a cradle position is fairly discreet, but I prefer the convenience of nursing my baby upright so that she can switch sides and doesn’t need to be taken out to be burped.
Thus, I’m loving my front cross carry for traveling!

Nursing in th FCC While Bagging Groceries (5 wks)
My baby is five weeks old and yesterday she stayed awake in the wrap while I did some grocery shopping.
Annabelle is almost always sleeping or nursing in the wrap. I think this is a sign that she’s growing up. She was awake and alert and I really enjoyed it!
Until now I’ve mostly had her wrapped low on my torso for easy access for breastfeeding. There was almost no point tightening her back up after nursing because she’d likely start rooting around for the breast again and need to be lowered. With such a little baby, wearing her low was not uncomfortable.
I think I’m going to start wrapping her high on my chest where she should be now, which is much nicer really: more cuddly and more comfortable overall.
Luckily I find that I don’t regret my babies’ growing up because they are so much fun as they grow up!
At five weeks old, Annabelle’s sleep routine is not yet predictable. We have better nights and less better ones. The biggest problem I’ve encountered is that after waking up to nurse, she sometimes doesn’t fall asleep again!
At times like these, I discovered that the one sure way to lull her to sleep, is to wrap her on my front and bounce on the birth ball pretty actively. If I keep it up for a good ten minutes she’ll be sound enough asleep to stay sleeping when I put her down in our bed.
While I’m VERY grateful to have this tool that works such a charm, getting up to wrap and bounce is a bit more of a disruption to my sleep routine than I care for! It would be great as a technique to put her to sleep at the beginning of the night, but that has not been necessary (she usually nurses to sleep while we watch a movie before bed).
Well, someone introduced me to the concept of swaddling and I instantly saw that a good wrap job is similar to a swaddle in that it surrounds the baby’s body with fabric, holds the baby tightly, keeps the baby’s limbs from thrashing around, and emulates the womb-environment. So it makes sense that they would have a similar calming and lulling effect.
Last night I swaddled Annabelle in a Miracle Blanket (loaned to me by my wonderful friend Evelyn) and she slept VERY well. When she woke up I was able to pull her legs out of the pocket in the swaddling blanket so that she could pee in the potty. Then I pulled the pocket back around her and nursed. When I lay her down, she went right back to sleep–awesome!

Annabelle swaddled, 5 weeks old
And wrapping to sleep . . . is still great for daytime! It’s wonderful to have other ways to parent Annabelle to sleep. Wrapping is a great way for fathers to provide comfort too.
I just used my 3.5 Neobulle Simon to put my five week old baby up in a high rucksack carry. I love it! The extra width of the Neobulle wrap made it real easy to get a good pocket under Annabelle, with plenty of width left to make a nice support behind her head. I’m thinking this is a really easy wrap to do a newborn rucksack with, especially for less-experienced parents!
The fact that the wide wrap is excellent for big kids to is a bonus–talk about one wrap for an entire childhood!
My photographer (Ada, aged five years) took these photos showing Annabelle after we wrapped up, and after she fell asleep (8 minutes later).

Neobulle Rucksack 9:25am

Neobulle Rucksack 9:33am
Since her head fell sideways instead of forward against my neck, I reached up with both hands to pull the top edge of the wrap higher behind her head and I did not have to retie anything:

Pulling the top of the wrap up for head support

Sleeping and Supported, 5 weeks old

4 weeks old, nursing in the FWCC
Soon I tried nursing upright in the wrap because I prefer wearing babies in the upright position, and because this position allows the baby to change breasts without the wrap having to be retied, and it is also the perfect position for burping.
I wrapped Annabelle upright, then lowered her down enough to put her mouth slightly higher than the level of my nipple. Then I just needed to make sure the parts of the wrap coming around her head were the perfect tension to hold her head right there. Then tie. I like the front wrap cross carry best for this, and the front cross carry works great too.

Nursing in the FCC, 1 week old
When nursing upright, Annabelle usually ends up slanted in a cradle/upright hybrid position. If she is nursing on the right side, then the wrap coming over my right shoulder is more bunched up, coming from behind her head to over my shoulder where it’s bunched away from my neck and right at the ball of my shoulder. The wrap going over the left shoulder is spread wide, covering Annabelle’s whole body and crossing the entire width of my shoulder to my neck.
In fact, I’ve found that my upright nursing carries sometimes end up looking like a cradle carry, though that wasn’t how I put her in! She won’t end up horizontal, but she does end up at various angles and rarely straight up and down. This is how it has worked out for us and it highlights for me the versatility of wrapping and the fact that you don’t need to worry about duplicating a precise position, but finding something that works well, even if it looks unlike anyone else’s version of a wrap job. So chill out, get your baby nursing and talk that wrap into holding baby in that position so you don’t have to!
The trickiest part of nursing in a wrap, with both cradle and upright positions, is getting the wrap to hold the baby’s head just right so you don’t have to. You have to realize that the wrap needs to do exactly the same job your hand or arm is doing when you hold the baby there, and the fabric certainly can be made to do that. Just persist in tightening or loosening or adjusting until you get it. A lot of adjusting can be done without taking your baby off the breast, and with your baby nursing, you may find you have uninterrupted time to get finicky with your wrap job!

Annabelle Nursing, 1 week old

4 days old, Nursing in a Hip Cross Carry
I began by nursing Annabelle in the cradle position. With a newborn, I found that intuitively I used the wrap to hold her against me in the same position that my arms held her when we nursed on the couch: cradle.
This was easier than I expected. I recommend doing it sitting down and using a front cross carry, front wrap cross carry, or hip cross carry–whichever method you are most comfortable and familiar with.
I’d begin wrapping around my baby, whom I held in the crook of my arm, then would latch her on before tightening and tying. I did find that I almost always had to adjust it again once, sometimes right away, sometimes a few minutes later.

1 week old, nursing FWCC
It usually worked best if the cross that goes over the shoulder on the same side she’s nursing on is bunched up behind her head. It can be spread across the baby’s body, but where it comes around baby’s head, bunching it behind provides a real sturdy support to hold the baby’s head at just the right angle.
And my baby, anyway, doesn’t like having anything covering her head, she prefers the behind-the-head method! You can see in the photo above that the wrap on my left side is going around and behind her head, rather than over it.
I’d find that while nursing was essentially hands free in that I could remove my hands from the baby and still be nursing, it felt more comfortable if I kept one arm around her holding her on. Luckily, it did not take long to observe that when I held her up with my arm, that made some slack in the wrap that, when tightened, replaced the function of my arm. I just took the slack out while holding her, retied, and then my arm was redundant and I could put it to use on other projects–like actually getting myself a peanut butter sandwich!

4 day old Annabelle Nursing
I was seven months into my second pregnancy, with many more discomforts than my first pregnancy, when my midwife asked me to get an ultrasound. Something just didn’t seem right, and she would be more comfortable if we checked it out.
We had the ultrasound and were joking together in the waiting room afterward, when the midwife came in and said soberly, “It looks like there are some malformations.”
“Oh my God,” I said, and looked at David. It was SO unexpected and such a shock that I didn’t really know if it was real. Once it sunk in, I started to imagine horrific malformations—a baby with two heads—and instead of feeling compassionately toward my baby, I found myself squeamish and grossed out that something malformed was growing inside of me. Suddenly instead of being a mother or a baby, I was a victim in Alien.
It did not help that the hospital could tell us nothing more. They sent us to another hospital where we were to get a level two ultrasound. We went the next day, and spent a good couple of hours trying to convince them to admit me. Apparently you can’t just waltz into a place and get an ultrasound. You have to have been sent by a medical professional. Well, we had been, but we hadn’t been given a piece of paper saying we had been.
At last we were in, and once they had administered the ultrasound they put on their serious faces and told me that I couldn’t leave. My baby had hydrops fetalis and the organs were not developing properly. I would have to stay in the hospital and the baby would be monitored constantly.
The next morning I was told that I would be getting a cesarean that day. The sooner the baby came out, the sooner the medical professionals could get to work fixing the baby’s body. It was our baby’s best chance at survival.
Being the last person in the world who would ever have a cesarean, I asked if there wasn’t some way I could birth vaginally. I was told that the baby was breech, and anyway wasn’t strong enough to survive being squeezed through the birth canal. I nodded numbly.
I almost told them how I didn’t want a hat put on the newborn baby because I had decided that being held skin to skin would provide enough warmth, and that I thought a baby’s body would learn to self-regulate temperature quicker without a hat; that babies were made to self-regulate when they needed to, and that their bodies are fast learners; that I didn’t want a hat to interfere with my smelling and nuzzling and bonding with my newborn. Then I remembered that they would be trying to save the baby’s life, to keep the heart beating, and that my crazy newborn hat ideas were pretty meaningless. I remembered that my baby might not live. And I kept my mouth shut on this most trivial of birth plan details—the only one that came to mind at the time. It hadn’t occurred to me to discuss whether my baby was bathed, or to request that she be kept with us, to mention my intentions to breastfeed exclusively or the fact that I didn’t want my baby circumcised. No, it was the hat thing that came to mind.
I treasure the few minutes we had to hold our baby girl, to name her and make sure she knew that we loved her. I really look back on this day fondly. It was the day I met my daughter and they only day I held and kissed her.
Those unmatched moments were preceded by a horrific operation. They kept increasing the anti-nausea influence pumped into my IV, and I kept vomiting anyway, so they gave up and handed my husband one of those little vacuums the dentist uses to suck the saliva out of your mouth. Thus were the mother and father engaged while the baby was being born. It was as if we were not at the birth. The birth happened on one side of the curtain, while my husband tried to comfort me through a terrible illness on the other.
They told me that I would feel as though I could not breathe, but not to worry because my body would be breathing just fine. I nodded at the time, but it turns out that when you feel like you can’t breathe, it’s very difficult to remain calm. I kept insisting that my collar was cutting into my neck and my husband and the anesthesiologist tried with futility to pull it away enough to make me comfortable.
I wondered if I would survive. I wondered how much longer I had to survive it. I forgot that a baby was being born.
Suddenly I realized that there were a group of doctors saying medical things on the other side of the room, and a second group of doctors murmuring over my body. I thought, the baby is out! Those doctors reading out heart rates aren’t talking about mine—I had a baby! I squeezed my husband’s hand and my eyes filled with tears. I don’t know when the baby had been born or how long until I noticed but I was a mommy and I no longer noticed whether I could breathe or remembered to vomit.
One of the doctors came over and wondered whether we wanted to be told the sex. Until now, even with all the ultrasounds, we had requested to remain in the dark. Suddenly the baby had been born and I realized there was no moment of revelation to wait for. Sheepishly I said that they could tell us the sex. I mean, hell, everyone else knew!
She was a girl. She was alive—I could still hear reports of her heart rate. She was going to be rushed to the neonatal intensive care unit and the father had to go with her. I could see her go by if I turned my head just so and waited.
They were wrong—I couldn’t see her. I only saw doctors and a wheeled table rush past. Then I was left alone. I guess they were still repairing me. I lay there for a long time not knowing what was happening behind the curtain but thinking about what might be happening in the NICU.
Finally I was wheeled into a curtained room to recover. Recovery meant a deceptively friendly nurse pushing down on my abdomen to cause uterine contractions. This was more painful than birth ever was. After a while family members were admitted one at a time. My mother and sister, and my husbands parents had all come to the hospital to wait outside the operating room. They knew that their opportunity to meet their grandchild might be brief.
One at a time they smiled at me and held my hand, and said nice things about our little girl. They had all seen her already. I guess she had been ready for visitors before I had been. We talked about giving her a strong name because she would have to be strong. Tiamat, my sister suggested. I told each of them that I knew she would be all right because our family was a strong and happy family that had good things happen to us. By now I was convinced that she would overcome the difficulties she’d had in utero and quickly grow into a healthy and normal girl. I believed in and expected a miraculous recovery. How could it be otherwise.
They each agreed with me in turn, but they were reserved.
Finally David came in to see me. He told me that I needed to come see the baby. He asked the nurse how soon I could see her. He didn’t say that he was afraid she would die before I got there.
Eventually I was wheeled through the hospital to the NICU. There were several babies in plastic boxes with parents hovering nearby. There were lots of wires and machines and blinking lights and blinking noises. And there was my baby, lying still, eyes closed. She was dark brown and a little bit purple and very big—she did not look premature. Her body was puffy and swollen beyond normal. She didn’t move.
I could touch her, and I did, reaching across from my sickbed to hers.
Hi, baby. I’m your mommy and I love you. I’m so happy to see you. You’re going to get strong and come home. Soon I’ll hold you and things will be much better. You need to be strong and get better, sweet baby.
I said these things, with my hand on her head, because it was the part of her that wasn’t covered up. I knew she needed a mother’s touch and a mother’s voice. My own mother was with me while I talked to her because girls need mothers.
David had been talking to the doctors and now came to get me. They took me into a closed room where we could have privacy, and David told me that her lungs, which had stopped developing months ago, would never develop the way they were supposed to.
While in my womb she had been healthy–I had felt her kicking strongly every day. In utero my body had sustained her and she had not relied upon her own organs. Outside the womb she would not live without life support. I was her mother and if I could have been her life support as I had been for more than half a year, I would have. But I couldn’t even hold her. I nodded calmly and said, “So we should turn off the machines?”
He nodded.
“Then can I hold her?”
He thought so, and the doctor confirmed it, and the fact that I would get to hold my baby made the decision so easy. Yes, take her off the machines and bring her to me!
Our family gathered in this room, and a doctor brought my baby to me and put her into my happy arms. I immediately started to unwrap the blanket around her so that I could see her body, but found that wires and syringes were wrapped up in it. I quickly covered her up again, because it was the opposite of how I wanted to see her.
I studied her face and this time I told her a different story. I told her that she could leave this body and find a healthy body. I told her this one hadn’t grown properly but that she could find another body that would be perfect and that she would live a wonderful life in a healthy body. I told her that life was really nice and that it wasn’t usually like this—hospitals and plastic boxes and blinking lights. I told her I loved her, and I would always be her mommy and she would always be a part of our family. I told her how glad I was that she had come so I could meet her. I told her we had decided to name her Clementine Annabelle.
Then her daddy and each of our family members held her and spoke to her. I asked for a camera and someone found one to take some pictures of her. Then the doctor came in and listened to her chest and told us she was gone and we let him take her body away.
David’s mother asked if I didn’t think she had perfect little ears and I worried because I hadn’t looked at her ears. Later I asked to see her body at the funeral home because I wanted to look at those ears. It was a mistake, as this empty body looked completely different, her mouth stretched downward at the edges in a frown that could only be made by uninhabited flesh. I quickly looked away.
We scattered Clementine’s ashes in the Gulf of Mexico. Ada misses the sister she never met. Recently, after the birth of our third daughter, Ada asked me why we didn’t bring her to the hospital to meet Clementine and I explained how unpleasant it had been and that we didn’t want her there unless we knew the baby was going to be okay. She named her doll Clementine and takes very good care of her. She waited patiently for us to get pregnant again so that she could finally meet a little sister, and she celebrated the birth of our next baby with a lot of joy.
Ada has been the most amazing sister and daughter. She takes good care of us and shows a lot of love every day throughout everything. She delights in her little sister, with no impatience, and is always there to hold her hand and say, “Don’t worry, little Apple,” when the baby is crying.
Our new baby shares a name with the one we lost. She is Annabelle Apple, perfect, and healthy, and surrounded by love.
Before we could get pregnant again, our family had to move out of mourning and come to a place where we could look to the future again with love, excitement, and a certainty that life is good. Babies need happy families, which is why they are blessed with the ability to make us so very happy. And now I think of each of my three birth-days with love and happiness.
I encourage anyone who has had a traumatic birth experience (regardless of the outcome) to address it fully and with all your heart before you next birth. Annabelle’s perfect birth in our home would not have been possible without our comfort with birth and our knowledge that this baby was healthy and this birth was not tied inexorably to the previous one.
We had to come to this knowingness in spite of the medical warnings and admonitions. We did a lot of research to determine why it was unsafe for me to birth vaginally and based on the studies, statistics, and our own experiences, we determined that a home vaginal birth was, in fact, the safest birth for me and our baby.
I did a purification rundown through my church which rid my body of the drugs that had been administered to me in the course of my hospital stay, and this program culminated with a miraculous few minutes in which all the mis-emotions of that birth experience spilled out of me and when they were gone I was left with peace. That same moment is when the tenderness on my abdomen vanished and the numbness left by the operation disappeared. I know from this experience that physical toxins, body somatics and emotions are tied together in a very real way that I believe contributes to physical problems that can occur in the future—such as uterine rupture or stalled labor leading to a cascade of interventions.
I also received counseling from my father, a minister, on the experience of Clementine’s birth and we continued until the experience left the realm of emotional trauma and came to be better described as a memory with loss about which I can be sad without being helpless to that sadness. I was myself again, only richer in knowledge and experience and love, instead of being a victim of what had happened to me.
In these ways I was prepared to conceive and birth again and I am so happy with the outcome. It allowed my daughter to have a healthy and safe birth free from fear or sadness, and allowed her to have a healthy, happy mother too.
I am deeply indebted to my husband who took such good care of me and makes me happy enough to withstand any devastation! He never faltered in holding my hand through this despite what he was going through personally as a father and husband.
Our family couldn’t have been more wonderful and we are very lucky to have so much support.
Without Jill Adams, who puts the “independence” back in “independent midwife,” we would not have had prenatal care and a trained birth professional. No one else here would entertain the idea of my birthing vaginally due to the “high risk” vertical incision on my uterus. Jill not only accepted me into her care without batting an eyelash, but after our initial discussion of emergency procedures should we need to go to a hospital, she did not bring up my scar, never referred to me as high risk, did not refer to a “trial of labor” and showed nothing but confidence that my homebirth was assured.
Dr Magloire, based out of Miami, drove the six hours to Orlando just to meet with several of us VBAC (vaginal birth after cesarean) hopefuls because there was no doctor closer than six hours away who would agree to discuss the risks and benefits of vaginal birth versus cesarean delivery and then sign a piece of paper saying we had been made aware of the risks.
In Florida this is a legal requirement for a midwife to deliver a baby vaginally to a woman with a scarred uterus. That’s right, I had to get permission to use my vagina. Why is it that “no means no” but when it comes to using my vagina for its intended purpose my right to assert that “yes means yes” is passed off to an OB?
I originally thought I would have to birth in a hospital. It was only after searching in vain for a doctor who would “allow” me to have a VBAC in a hospital that I started to wonder whether I had a chance at a homebirth—my first choice.
But was it safe? I researched heavily and in the end the truth found in my heart was more important than truth found in statistics. I’m convinced that uterine rupture (the big risk of vaginal birth after cesarean) is more closely linked to spiritual and emotional than physical state, not because the integrity of the uterus is not important but because the physical follows the spiritual. Form follows function. I’m not proposing that it’s all about confidence, or being prepared. But I think fears are very important to the VBAC and that coming to peace with the past is probably the greatest contributor to success. Birth is such a sacred event and going into it with anything less than a full measure of strength and peace is dangerously irreverent.
I did have to come to terms with the statistics as part of the process of gaining peace. Other mothers with a classical incision may find it difficult, as I did, to understand “their chances” because of the amazing dearth of information on the VBAC with a classical incision. This incision type is very unusual now, so that all the literature reassures mothers that unless you have a classical incision, the risk of rupture is really very small. That left me saying, “But what if you do have a classical incision? What then? Is there no hope?” And the literature doesn’t give any clue.
The information here gave me hope: http://emedicine.medscape.com/article/275854-overview.
A 2% rupture rate was not so high. And I did not have any information about the health, weight, diet or spiritual state of any of the women in the study. I reasoned myself to be healthier than most Americans, physically and emotionally, and concluded that my risk of being in that 2% was itself small. Add to that my advantage of having had a prior vaginal birth, and the fact that it would be two years between births. Most compelling, I planned a large family, and all the studies show that the more vaginal births you have after cesarean, the lower your risk of rupture, while the more repeat Cesareans, the higher the risks of dangerous complications.
Furthermore, I reminded myself that a 2% rupture rate did not mean a 2% incident of fetal mortality. Outcomes were best when a woman with a rupture could be gotten into an operating room within about ten minutes. Our home is very close to a good hospital. Close enough that getting to the operating room might take no longer for me than for someone in the labor and delivery ward of the hospital itself! I called the hospital to verify that they are in fact ready to operate at all times with anesthesiologists, O.R.s, and surgeons on hand.
I had come to realize that for me, birthing in a hospital would mean major abdominal surgery. So I decided to birth at home, and plan on going to the hospital only in the event that I needed that surgery.
Another tangent to research is the laundry list of risks associated with cesareans in general and repeat cesareans in particular. The 2% risk of rupture was not after all weighed against a 100% guaranteed complication-free cesarean birth. To the contrary, I found benefit after benefit of birthing vaginally, for both the baby and the mother.
I told my husband how sure I was about having a homebirth, assured him I would not risk our baby’s life and that my choices were being made in order to secure the best outcome for our baby. My husband told me that after one homebirth and one hospital birth, the last place he wanted us to go was a hospital. He much preferred a homebirth, a safebirth.
So I was ready to hire a midwife. Unfortunately, the search for a midwife mirrored my search for an obstetrician—this one, too, seemed destined to failure. I was contemplating going out of state for my birth when someone on the local ICAN (International Cesarean Awareness Network) recommended Jill Adams. They didn’t know if she would accept a client with a classical incision, but she was known for accepting higher risk mammas. Lucky for me, Jill had just started her own business as an independent homebirth midwife after working at a birth center for a woman with more conservative views.
We met with Jill who explained that we would have to get our permission slip signed, but assured us that she would be happy to attend our birth with that legality out of the way. She wanted us to get one ultrasound to verify the position of the placenta, but she was willing to forgo use of the doppler during my prenatal care and resort to her old-fashioned fetoscope so as to minimize our baby’s exposure to ultrasound. She was experienced with vaginal birth after cesarean, and with home waterbirth. She was confident, comfortable, friendly and wonderful with our five year old daughter, whose presence was welcome at the birth along with whoever else we wanted there.
And she does this for families all the time.
The story of our perfect, peaceful homebirth on Christmas Day 2009 is here.
So it’s a mom’s gathering, and babywearing is one many topics that come up. But my focus is on baby wraps: showing them to moms, helping moms with them, getting to touch and play with other people’s wraps . . .
We meet every Wednesday morning (11am) at the Labor of Love in Dunedin Florida. Frankly the room is getting too crowded, but it’s fun to meet all the moms and babies!

Looking Beautiful in the Ring Sling

Wearing two: infant and toddler at once!

First Wrap Job - Elsa EllaRoo

Wrapping faster than the eye can see--and just look at those newborn feet!
Perhaps blogs are not supposed to have a point. But I didn’t have a Wrap Your Baby Blog, and now I do. The reason is that I have wrap related thoughts throughout each week that I think are worth mentioning, could be helpful, or others might enjoy.
With a baby coming around Christmas, I know I will be wrapping daily and I’d like to share my experiences through the seasons, while traveling, at different ages, and for different occasions or needs.
Besides, it is important to me that news of babywearing get out there. I want all new parents to know about baby wraps. This is my contribution toward that end!